Marissa Schlueter of OMERS Ventures posted a comment on spotting next generation healthcare opportunities:
Here’s a radical understatement: The last couple years have been tough.
But
— at least for me personally — tough times also provide the opportunity
for reflection and change. Going into 2022, I have a much better sense
of who I am, what I value, how I learn and where I want to be. And
that’s as a health tech investor at OMERS Ventures.
I’ve
long entertained venture capital as a potential career in the back of
my mind. Now feels like the ideal moment. I’m hoping to take my
experience with public equity research at Melius Research, as well as
private company research at CB Insights to help trend spot and identify
the next generation of opportunities in health-tech.
Why VC?
For years, friends and family have joked that I’m a professional student — and they’re not wrong.
My
previous roles have relied on my ability to consume large amounts of
data, synthesize actionable insights and communicate those learnings to
key stakeholders as they evolve. VC gives me a perfect forum to do what I
do best in service of finding great founders and helping them build
their businesses.
As
nerdy as this sounds, I’m genuinely excited to help founders build and
refine their financial models, dig into user and company performance
metrics, conduct competitive and market landscaping analyses, and
identify strategic growth opportunities.
I’ve
also come to realize how much I value purposeful, mission-driven work.
At the micro level, this affords me the opportunity to really make an
impact on entrepreneurs making healthcare better. After all, when they
win, we all win.
Why OMERS Ventures (OV)?
I should start by explaining what OV is.
For
the uninitiated, OV is the VC arm of OMERS (Ontario Municipal Employees
Retirement System), one of Canada’s largest pension plans with around
$100B in net assets. With teams in Toronto, London, and Palo Alto, OV
makes multi-stage (Series A to C, with the occasional, exceptional Seed)
investments in growth-oriented startups across North America and
Europe.
As
is often the case in venture, people are paramount, and I knew I
couldn’t make the jump with just anyone. Specifically, I wanted a team
with a strong culture of collaboration, mentorship, and diversity. It
was also important for me to join a team that viewed their portfolio
companies as valued partners instead of strictly as investments.
Where I’m rolling up my sleeves
Below are just some of the health tech themes, segments, and end markets I look forward to digging into as a VC.
Many
of these are personal to me — I’ve either experienced the problem
firsthand or have dear friends and family members who have. They also
overlap with what I’ve observed (during the last few years at CB
Insights) as relatively under-appreciated pockets of opportunity for
tech integration and advancement.
If you’re a founder focused on any of these areas, reach out to me at mschlueter@omersventures.com — I’d love to learn more about what you’re working on.
– — — — –
Wraparound care
A
growing number of startups are using digital technology to productize
supplementary health/social services and integrate them into next-gen
care delivery models. These wraparound services — which may include
coaching, social counseling, dietetics, companionship, peer/community
support, navigation, coordination, education, prescription management,
transportation assistance, etc. — aim to enable more holistic,
personalized, seamless and higher-quality care.
While
covering the telehealth space at CB Insights, I saw many point
solutions being used for distinct applications/populations, including
lifestyle coaching for type 2 diabetes prevention (e.g. Lark Health,
Noom), companionship for aging seniors (e.g. Papa), and peer support for
recovering addicts (e.g. MAP Health Management, Marigold Health).
But
given increased focus on social determinants, shifting consumer
expectations, and expansion of verticalized virtual care delivery, I
think this trend is in its early innings.
Over
the next few years, I expect digitally-enabled wraparound care to
become more commonplace and also more comprehensive as next-gen care
models emerge for specific demographics (e.g. age, gender, race,
socioeconomic status, sexual orientation, etc.) and medical conditions
(e.g., cancer, CKD, IBD, HIV/AIDs, etc.).
In
the near-term, I’ll be keeping a particularly close eye on the
integration of mental/behavioral health and peer/community support into
care for patients with rare, complex, debilitating, life threatening,
and stigmatized conditions.
In
response to the pandemic, many health systems, patients, families, and
even clinical trial sponsors/CROs increasingly sought out home-based
alternatives for care traditionally delivered in institutional care
settings like hospitals and skilled nursing facilities (SNFs). But while
the shift to home-based healthcare was accelerated by the pandemic,
there are several reasons it could persist.
“Hospital-at-home” (HaH) for acute & post-acute care:
A growing body of research supports HaH’s ability to demonstrate
material cost savings, reductions in readmissions and lengths of stay,
and improvements in clinical outcomes and patient satisfaction ratings.
CMS has also signaled a willingness to reimburse for Medicare HaH
services during the public health emergency (PHE) with the
implementation of the Acute Hospital Care At Home waiver program. Though
there are some issues to be sorted out, the program is a move in the
right direction from a reimbursement angle and industry stakeholders (Advanced Care At Home Coalition) are aggressively advocating for its extension beyond the PHE.
The startups highly levered to this shift are raising some serious capital:Medically Home just announced a $110M Series D led by strategic investor Baxter International, and last year, DispatchHealth raised $200M in Series D financing at a $1.7B valuation. We’re also seeing M&A activity here: Admedisys picked up Contessa Health for $250M and Best Buy acquired Current Health for $400M.
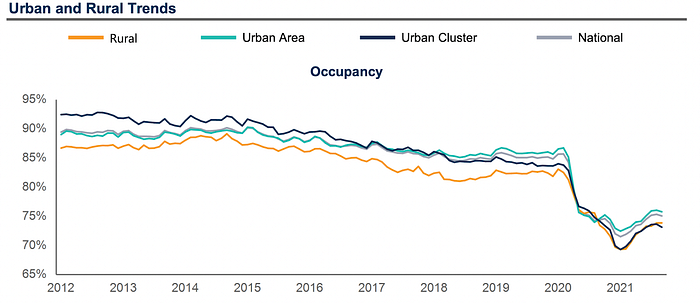
Extended care for aging and disabled patients: Aging
and disabled patients and their families have been shifting away from
SNFs in favor of home-based care for the better part of the last decade.
The pandemic only accelerated that trend. Though SNF occupancy has
bounced back slightly from its all-time low (early 2021), the pace and
magnitude suggest we will not be seeing 85%+ occupancy again for quite
some time… if ever.
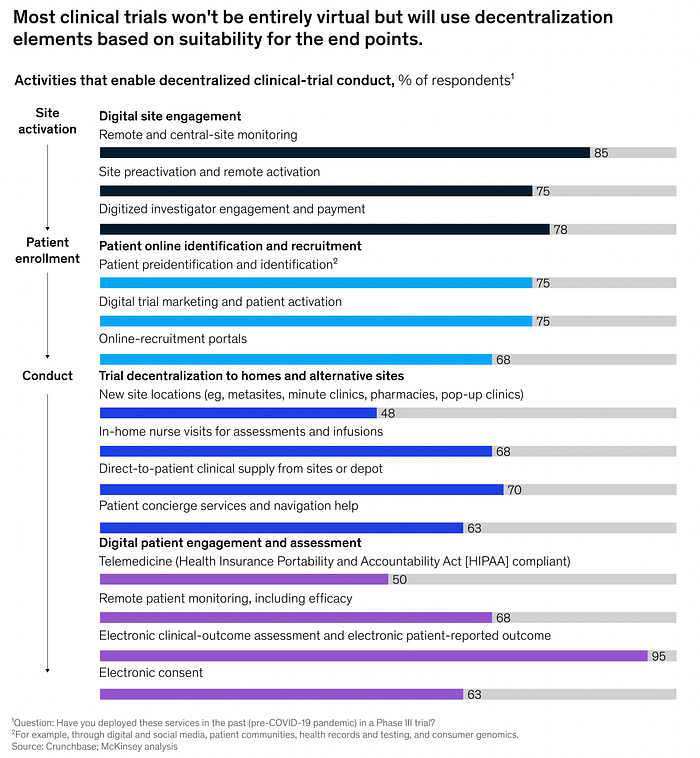
Decentralized clinical trials (DCTs): During
the pandemic, mass decentralization happened out of necessity. But the
tech demonstrated valuable benefits: it allowed clinical trial
investigators to reach larger, more diverse patient pools, work more
efficiently, reduce participant dropout, and generate cost savings for
sponsors. Having had that experience, the vast majority of clinical
trial sponsors and CROs expect virtual trials to be a big component of
their portfolios going forward, with most activities conducted in
participants’ homes (according to a McKinsey survey).
For
any/all home-based care programs/paradigms, tech will be absolutely
critical to the economics, clinical impact, and patient experience —
from identifying eligible participants, to coordinating care, optimizing
staffing & logistics, remotely monitoring patient vitals &
self-reported symptoms, and more.
While
at-home Covid testing may be the most immediately relevant application,
the overarching market opportunity for decentralized testing is much
more expansive.
We’re
already seeing at-home testing solutions tailored for routine
screening, high-risk screening (CKD, prediabetes), fertility screening
(male & female), low acuity diagnostics (UTIs, STIs, common
respiratory viruses, food sensitivities), and even pharmacogenomics
(birth control selection).
I
expect this list to expand, especially as more care is delivered in the
home (acute/post-acute, aging-in-place, clinical trials, etc.) and on
the back of some material business developments over the last year or
so.
The
interest is coming from all angles of the market — we’ve seen: virtual
care providers bolting on at-home testing assets (Ro’s acquisition of Kit), at-home testing players acquiring virtual care businesses (23andMe acquiring Lemonaid Health), traditional diagnostics giants getting their foot in the door (BD’s acquisition of Scanwell), and digital infrastructure being built to support the trend (Truepill’s diagnostics launch).
But
even beyond at-home testing, there are tremendous opportunities to
bring diagnostics closer to the POC — whether that’s in an exam room, at
the patient’s bedside, in a community health center, at a retail
pharmacy, etc. — because doing so significantly reduces test turnaround
time (compared to sending samples out to a reference lab), which in turn
can shorten treatment response times, improve patient outcomes, and
reduce costs. This is particularly critical for conditions like sepsis
and hospital-acquired infections.
Digital pharmacy & DME fulfillment
Digital pharmacies like Capsule, Medly, and Alto
have been around for several years but the pandemic really catapulted
their growth. The same goes for DTC virtual care/pharmacy fulfillment
(“telepharmacy”) companies like Ro, Thirty Madison, Nurx, Pill Club, etc.
Again,
I think this phenomena will outlast the pandemic. And so do major tech
& retail players: for example, Uber has partnered with ScriptDrop
and Amazon and Walmart launched their own digital pharmacy offerings.
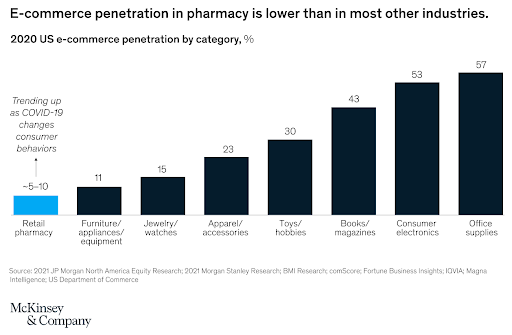
So, why the optimism?
The opportunity is massive. According to McKinsey,
only 5–10% of the US retail pharmacy market ($460B) happens online.
That’s less than half the penetration rate seen in other industries like
apparel, consumer electronics, and office supplies. While some drug
classes are legally prohibited from being prescribed online (per the
Ryan Haight Act), enforcement was relaxed during the PHE and some think we could see a permanent reversal of the law in 2022.
2.
Consumers increasingly demand convenience. The proliferation of digital
health services during the pandemic has given consumers more power in
choosing where/when/how they receive care. And when the choice exists,
consumers will always choose the more convenient option, all else equal.
Once in place, these expectations are very hard to reverse, and for
those reasons I think digital pharmacy/direct-to-patient medication
delivery will only grow in demand.
3.
More care is happening at home. New opportunities for digital pharmacy
will emerge as more care shifts out of institutional care settings and
into patients homes. Patients who would normally get their medications
on-site at a SNF, for example, now need a different service to fill that
gap — for disabled patients or those who no longer drive, digital
pharmacy/home delivery is a perfect fit for that.
Another
tangentially related area I’m interested in is tech improving durable
medical equipment (DME) logistics & fulfillment. Roughly 1 in 4 US
seniors rely on DME in some way but getting and maintaining it can be a
very confusing and complicated process for those living at home.
Companies like Tomorrow Health and Better Health
are using tech to improve stakeholder connectivity, optimize supplier
matching, streamline order & refill processes, and improve
transparency & patient choice.
Caregiver support & empowerment
According to the National Alliance for Caregiving
(NAC), a greater proportion of US adults are taking on unpaid
caregiving responsibilities each year. In 2020, 21.3% served as a
caregiver to a family member or friend compared to 18.2% in 2015. On top
of that, a greater proportion are providing care to 2+ people: 24% did
so in 2020 vs. 18% in 2015.
The NAC attributes these findings to:
“The increasingly aging baby boomer population requiring more care
Limitations or workforce shortages in the health care or long-term services and supports (LTSS) formal care systems
Increased efforts by states to facilitate home- and community-based services
Increasing
numbers of Americans who are self-identifying that their daily
activities, in support of their family members and friends with health
or functional limitations, are caregiving
Regardless
of the causes, we’re witnessing a “caregiving crunch” that’s only
projected to grow more acute in the future. According to Lisa D’Ambrosio,
a research scientist at the MIT AgeLab, “shifting demographics will
lead to a drop in what’s known as the caregiver support ratio: the
number of adults ages 45 to 64 who are available to provide care to
those 80 and older. Between 1990 and 2010, the caregiver support ratio
hovered at around 7 caregivers per care recipient, but by 2030 the ratio
is estimated to decline to 4 to 1, hitting 3 to 1 by 2050.”
Tech
is unlikely to solve this problem entirely but it certainly could have
outsized impact on low-touch caregiving activities like social
engagement/companionship, medication management, care coordination,
transportation & meal assistance, etc. DUOS,
which emerged from stealth in 2021, is an interesting example as it
pairs aging adults with dedicated personal assistants to help with these
“social determinants of aging,” leaving high-touch activities to be
managed by caregivers.
I’m
also interested in businesses looking to support caregivers’ mental
health and wellbeing. One company integrating mental/emotional health
within a broader suite of caregiver support tools is ianacare, which just recently raised $12.1M in Series A financing.
Palliative care
Contrary
to popular belief, palliative care is not synonymous with hospice and
isn’t exclusively meant for the very elderly or terminally ill. Though
it was originally developed for those purposes, palliative care has
evolved into its own medical speciality that caters to people of all
ages and all types of serious medical conditions including heart
disease, AIDS, MS, stroke, liver disease, and more.
Instead
of treating underlying conditions, palliative care teams — a
multidisciplinary mix of physicians, nurses, social workers, mental
health professionals, and chaplains — focus on alleviating patients’
symptoms and meeting their emotional, spiritual, and quality of life
goals. They also serve as critical support systems for patients’
families and caregivers and as care coordinators with patients’ primary
physicians. Importantly, unlike hospice, palliative care can be — and
often is — delivered alongside curative or life-prolonging treatment.
Studies
have consistently demonstrated palliative care’s ability to drive
meaningful improvements in quality measures, resource utilization, and
costs. As a result, it’s been one of the fastest growing
fields in medicine. Between 2000 and 2016, the percentage of 50+ bed
hospitals with a palliative care team tripled from just 25% to over 75%.
Despite its growth, palliative care remains underutilized. Roughly 60% of people who would benefit don’t get it. Two of the biggest reasons have been consumers’ lack of awareness and physicians’ hesitation to initiate discussions with their patients. But those things are beginning to change
— and demand is rising — in response to the pandemic. Telemedicine has
also begun to alleviate some of the access and supply shortage
challenges (e.g. Vynca, Devoted Health, Mettle Health).
But as utilization picks up, there will be greater need for other digital health tools
to improve patient/family/caregiver education,
patient-provider-palliative care team information sharing and
communication, symptom management, advance care planning, family
grief/bereavement counseling, and more.
Unique solutions for HCP shortages & burnout
Skilled
labor shortages and rising burnout have long plagued the US healthcare
system but, now with omicron, are growing increasingly more acute by the
day. Presently, the healthcare workforce is on the brink of a “Great Resignation,” which could send deleterious ripple effects throughout the entire healthcare system.
Despite
all the progress we’ve seen in health tech, in aggregate, these
innovations have failed to make a difference on the very people the
system depends upon.
Many
virtual care companies, for example, claim that they’re helping address
HCP shortages, but in my opinion they’re more so reshuffling when/where
the available HCPs dedicate their hours. Tech-enabled workflow
efficiency gains will only move the needle so far — maybe allowing them
to see a few extra patients per day on the margin. To fundamentally
address the supply shortage, we need to see more dedicated investment
into training and upskilling.
I’m also eager to see tech that improves HCPs’ quality of work life — e.g. by reducing information/tech overload (e.g. Wellsheet), relieving them of documentation duties (e.g., DeepScribe, Suki), providing intuitive clinical decision support, guiding them through difficult conversations, helping them develop stronger relationships with patients, instilling a sense of purpose, etc.
There’s
not going to be one fix-all, of course. But hopefully, in time, a
confluence of health tech solutions can help turn this ship around.
Provider directories & care navigation
I’ll keep this one short because my colleague Chrissy Farr sums it up nicely in her blog post here.
There’s one thing I’d like to add to her analysis:
Until
recently, provider directory and care navigation tech focused mostly on
the employer market, but the need for these solutions is becoming
increasingly relevant to the masses now that DTC health services are proliferating.
As
competition heats up, consumers will grow more discerning of where
they’d like to spend their out-of-pocket dollars. Beyond price, DTC
providers will be increasingly assessed for things like wait time,
cultural competency, ancillary services (e.g. prescription delivery,
at-home labs, etc.), patient reviews, etc.
Prior authorizations / utilization management
There
are two main types of waste that cost the healthcare system $1.1T
annually: administrative waste ($700B) and clinical waste ($445B).
Over
the last decade, a lot of time, money, and energy has been spent on
addressing administrative waste — understandably, since it’s a bigger
piece of the pie — but disproportionately fewer resources have been
devoted to tackling clinical waste.
We’re
starting to see that change. A growing number of startups are now using
tech to improve prior authorization processes and, ultimately,
utilization management. Some examples include: Olive, Cohere Health, and Banjo Health.
Medicaid—
Investment into Medicaid-focused businesses has historically been
limited due to concerns about scalability and profitability. But many of
these concerns are actually rooted in misconception. With Medicaid enrollment at record-level highs (almost 25% of the US population) and the rest of the healthcare system “[speeding] up its digital transformation by 10 years,”
it’s irresponsible to ignore technology that could make healthcare more
equitable, affordable, and accessible for a population that’s long been
overlooked and underserved.Cityblock
has been a standout for several years now but we’re only just beginning
to see other types of Medicaid-focused businesses emerge, like Circulo Health and Waymark.
Specific cultural communities —
There’s growing appreciation of the need for culturally competent HCPs
and healthcare organizations, with a wave of health tech companies like Hurdle Health, HUED, Health in Her Hue, and Pride Counseling emerging and established players like Grand Rounds/Doctor On Demand (now renamed Included Health)
acquiring culturally-competent businesses. Companies that specialize in
cultural competency education, training, and credentialing (e.g., Violet) will likely play important roles as this recognition grows.
Children & adolescents —
Pediatric health tech businesses have been in vogue recently, but
really just in one area: mental/behavioral health. There’s so much else
that goes into childhood development that’s not getting much attention.
I’d be interested in seeing health tech businesses working on pediatric
nutrition/healthy eating, allergy & immunology, endocrinology,
reproductive/sexual health, and sleep medicine. I’m also interested in
companies working on improving urgent & primary care in school
settings.
Women — Again, I’ll leave this one to Chrissy. This is a topic both of us are passionate about so will continue to be a big focus of ours going forward.
Specific conditions & specialties
To
avoid going down a million other rabbit holes (I’ll save that for
another time…), here’s a short laundry list of specific conditions and
medical specialties I want to dig into. None of these are truly
uncharted territory from a health tech point of view but they do likely
have pockets of untapped opportunity and definitely have areas in need
of improvement.
If
you’ve got unique experience, perspective, or intel on any of these and
how technology could play a bigger/better role in the future, please
reach out.
Pediatric
oncology — e.g., solutions to help parents/families to navigate care,
communicate with care teams, receive emotional support/counseling, etc.
Fertility — e.g., businesses aiming to improve the success rate and affordability of fertility care
So
as you can tell, this is a fairly exhaustive list. And I had to hold
myself back from including more. If you’re working in any of these
areas, I’d love to hear from you!
This is a fantastic, in-depth comment from Marissa Schlueter of OMERS Ventures.
She really covers a lot of the important trends and goes into detail (you can read more about the challenges and opportunities in healthcare here).
I read it last week and started following her on Twitter here.
OMERS Ventures is the venture capital (VC) arm of OMERS. With teams in Toronto, London, and Palo Alto, it
makes multi-stage (Series A to C, with the occasional, exceptional Seed)
investments in growth-oriented startups across North America and
Europe.
You can view all their investment, operational, legal and finance professionals here and the team is led by Michael Yang, Managing Partner out of the San Francisco.
I like their thematic approach to investing. They understand the big macro trends and focus on investing in high growth disruptive companies making an impact of various sectors of the economy.
But understanding big macro themes and making money investing in venture capital are two entirely different things.
I want to make it very clear, investing in venture capital was always and will be always be difficult.
First, competition for talent is intense.
For example, VC heavyweights including Sequoia, Bessemer Venture Partners, Lightspeed
and General Catalyst have all either opened new offices in Europe or started
notable expansions in the last 12 months. Hussein Kanji, co-founder of Hoxton Ventures in London, told CNBC that
the big US VC firms are finding it “super, super hard” to hire the
right people in Europe.
Also, the era of cheap money is coming to end and with that, a lot of speculation that drove hyper-growth tech stocks, meme stocks and cryptocurrencies to the moon has come to an end.
If these "super bubbles" are bursting and tech stocks enter a bear market, it will make it that much tougher for VC funds to realize on their investments because the IPO window will close.
This doesn't mean that OMERS Ventures can't compete, it most certainly can and will compete, it just means the environment is becoming that much harder for anyone investing in venture capital.
This is why the investment process in venture capital is critical as is extreme discipline.
Now more than ever, you need the right internal team, the right external partners and the ability to execute on a sound strategy.
Still, whether it's healthcare, the energy transition or other new or traditional sectors, venture capital is critically important for all of Canada's large pensions, they need to invest in tomorrow's disruptive technology companies to realize on their long-term return targets.
On a related topic, Bruce Power, a holding company of OMERS Infrastructure, announced today that it is forming a partnership with Isogen, paving way for production of life-saving medical isotopes:
Bruce Power and Isogen (a partnership between Kinectrics and
Framatome) have completed the installation of a groundbreaking Isotope
Production System (IPS), making Unit 7 the first power reactor in the
world with installed capability to produce Lutetium-177 (Lu-177).
Lu-177 is a medical isotope used in the treatment of various cancers,
such as neuroendocrine tumours and prostate cancer. In the future, this
system will also have the ability to produce other isotopes for medical
uses.
“This installation of the IPS is an exciting milestone on our journey
to becoming the first power reactor in the world to provide a scalable,
game-changing solution in the supply of life-saving medical isotopes
for the global medical community,” said James Scongack, Bruce Power’s
Chief Development Officer and Executive Vice President, Operational
Services. “Our medical isotope program and the IPS installation are a
result of years of innovation and development in partnership with
Isogen, Saugeen Ojibway Nation, and ITM, and will provide large-scale
capacity to help produce medical isotopes, which will be used across the
world in new treatments to fight cancer.”
With the new system now installed, activities will shift to planned
commissioning along with preparation activities for commercial
production that will follow once these activities and regulatory
submissions are successfully completed.
“Ontario is leading the way in the production and supply of medical
isotopes around the world,” said Hon. Todd Smith, Ontario’s Minister of
Energy. “I’m proud of the innovative work being done by Bruce Power and
its partners in the supply chain, including Framatome and Kinectrics.
Their efforts are helping to further cement our position as an
international isotope superpower, while providing critical medical tools
to help meet the needs of patients battling cancer.”
Lu-177 offers doctors an alternative to traditional chemotherapy by
deploying a “seek-and-destroy” dose to target cancer cells, while
limiting damage to surrounding healthy tissues and organs.
The IPS was developed and manufactured by Isogen, a joint venture
between Framatome and Kinectrics, which is focused on developing
innovative isotope production technologies.
“The installation and successful transfer of the first target marks a
major accomplishment and successful implementation of Framatome
Healthcare technology; the first Isotope Production System in a power
reactor for commercial production of therapeutic medical isotopes,” said
Curtis Van Cleve, President and CEO of Framatome Canada Ltd. “We
applaud the dedication and efforts of our partners at Bruce Power,
Saugeen Ojibway Nation, Kinectrics, ITM and our team, and the support of
their families that allowed them to see this installation through.”
“The installation of the IPS is the result of countless hours of
support from many people at Bruce Power, Framatome, Kinectrics, Saugeen
Ojibway Nation and our suppliers,” said David Harris, CEO of Kinectrics.
“The entire team demonstrated tremendous dedication, especially during
the pandemic. This was a critical step to enable the production of
Lutetium-177 for our partner, ITM, and to fortifying a strong, reliable,
and large-scale global supply chain of life-saving isotopes, that both
physicians and patients can depend on.”
With its new IPS system, Bruce Power will conduct the irradiation of Ytterbium-176 (176Yb) as a first step in the production of no-carrier-added Lutetium-177 (n.c.a. 177Lu).
Processing of the irradiated Ytterbium-176 for the production of n.c.a.
Lutetium-177, as well as the global supply of n.c.a. 177Lu, will be handled by ITM Isotope Technologies Munich SE (ITM),
a leading radiopharmaceutical biotech company that is one of the
largest and most reliable producer of Lu-177 for pharmaceutical use.
“The successful installation of this production site builds an
important milestone in our partnership with Bruce Power and Isogen to
scale up the production of high-quality medical radioisotopes,” said
Steffen Schuster, CEO at ITM. “We look forward to the upcoming launch of
the IPS and are proud to contribute with our unique manufacturing
methodology to yield high-quality n.c.a. 177Lu and to make it accessible for cancer patients worldwide.”
The installation of the IPS is a significant step in the landmark
isotope project, which is a partnership that began more than three years
ago with over 400 dedicated professionals working on various stages of
the project.
In November 2021, Bill Walker, MPP of Bruce-Grey-Owen Sound,
introduced a Private Member’s motion – which passed with all party
support – to assert Ontario’s leadership role in the production and
supply of medical isotopes as a strategic priority for the province.
Today’s announcement exemplifies that Ontario continues to be the
forefront of medical isotope technology.
“I want to congratulate Bruce Power, Framatome and Kinectrics on this
important accomplishment,” said MPP Walker. “Ontario has long been
looked to as a leader in the medical isotope space, and these partners
are playing an important role in the global supply chain to provide
patients around the world with life-saving cancer treatments and
diagnostic tools.”
Bruce Power will market the new isotope supply in an historic
collaboration partnership with Saugeen Ojibway Nation (SON). The
partnership project with SON, named “Gamzook’aamin Aakoziwin,” includes
an equity stake for SON and a revenue-sharing program that provides a
direct benefit.
“From the initial concept in 2019 to production expected in 2022, our
Gamzook’aamin Aakoziwin project is on track to meet an ambitious
timeline to have isotope supply ready to meet the increasing demand from
doctors and cancer patients around the world,” said Chief Lester
Anoquot, Chippewas of Saugeen First Nation. “Saugeen Ojibway Nation is
proud of the part we have played and will continue to play in this
project.”
“Short-lived medical isotopes are essential tools for doctors and
researchers in the fight against cancer, and this project will provide a
much-needed source of these isotopes for patients close to home, in our
communities, and around the world,” added Chief Veronica Smith,
Chippewas of Nawash Unceded First Nation.
“Thanks to the investments being made into the Bruce Power site
today, we can look to the future and realize a vital role in providing
life-saving medical isotopes to the world, while also supplying clean,
reliable and low-cost electricity to Ontario, growing the economy and
fostering innovation for decades to come,” said Hon. Lisa Thompson,
Minister of Agriculture, Food and Rural Affairs, and MPP for
Huron-Bruce.
You can learn more about how Bruce Power is helping to keep hospitals safe, and also diagnosing and treating cancer at www.brucepower.com/isotopes.
About Bruce Power Bruce Power is an electricity
company based in Bruce County, Ontario. We are powered by our people.
Our 4,200 employees are the foundation of our accomplishments and are
proud of the role they play in safely delivering clean, reliable,
low-cost nuclear power to families and businesses across the province
and life-saving medical isotopes around the world. Bruce Power has
worked hard to build strong roots in Ontario and is committed to
protecting the environment and supporting the communities in which we
live. Formed in 2001, Bruce Power is a Canadian-owned partnership of TC
Energy, OMERS, the Power Workers’ Union and The Society of United
Professionals. Learn more at www.brucepower.com and follow us on Facebook, Twitter, LinkedIn, Instagram and YouTube.
About Isogen
Isogen is a joint venture between Framatome and Kinectrics,
whose mission is to enable the use of CANDU reactors to produce the
medical isotopes needed to treat and diagnose patients with serious
diseases world-wide. Isogen’s enabling partnerships with Bruce Power and
ITM allows us to produce the world’s largest and most reliable supply
of life-saving, short-lived, therapeutic medical isotopes.
About ITM Isotope Technologies Munich SE
ITM, a radiopharmaceutical biotech company, is dedicated to providing
the most precise cancer radiotherapeutics and diagnostics to meet the
needs of patients, clinicians and our partners through excellence in
development, production and global supply. With patient benefit as the
driving principle for all we do, ITM is advancing a broad pipeline,
including two phase III studies, combining its high-quality
radioisotopes with targeting molecules to develop precision oncology
treatments. ITM is leveraging its leadership and nearly two decades of
radiopharma expertise combined with its worldwide network to enable
nuclear medicine to reach its full potential for helping patients live
longer and better. For more information please visit: www.itm-radiopharma.com.
Quite impressive, Bruce Power is an incredible company, a true leader in nuclear power generation, medical isotopes and more.
And it's an important holding of OMERS and its members.
Below, Startup Health sat down with Chrissy Farr, a health tech investor at OMERS Ventures,
where she focuses on women’s health and behavioral health.
In this
interactive chat, Chrissy talked about her priorities for the remainder
of the year, including focus areas of women’s and behavioral health, as
well as her experience making the change from being a full-time
journalist covering the health-tech beat at major publications like CNBC
and Fast Company to a venture capitalist, and how that has impacted her
view on company storytelling. She also gave the inside scoop on OMERS
Ventures and how to position yourself to get on her, and the broader
company’s, radar.
Second, Eric Kimberling, CEO of Third Stage Consulting, discusses the changes and challenges facing the healthcare industry and how technology is driving improvement for healthcare.
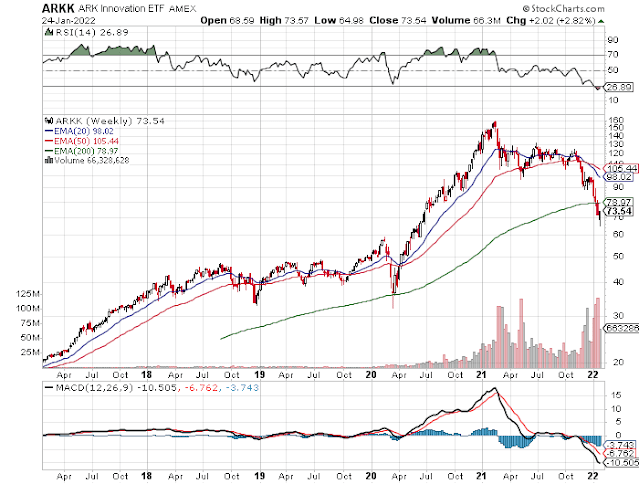
I also embedded an older CNBC clip on whether telemedecine is the future. It's interesting for two reasons. It shows you how the pandemic only intensified a trend but it also shows you how much hype was built into these stocks, many of which have been clobbered over the last six months.
Lastly, Linda McLachlan interviews John Ruffolo, founder of OMERS Ventures and founder of Maverix Private Equity. John is inspirational and truly incredible. Listen carefully to his wise insights and why you should say what you mean.

Comments
Post a Comment